Tailoring Systemic Therapy to the Clinical Domains of Psoriatic Arthritis
Reviewed by: HU Medical Review Board | Last reviewed: June 2026 | Last updated: June 2026
Key Takeaways:
- Both GRAPPA and EULAR organize PsA therapy by clinical domain; the goal is one agent that covers as many active domains as possible.
- Axial and skin involvement discriminate most sharply between drug classes, so they should carry the heaviest weight in selection.
- When domain coverage is comparable, comorbidities (IBD, uveitis, cardiovascular, and malignancy risk) should break the tie.
Few inflammatory diseases punish a one-size-fits-all approach as reliably as psoriatic arthritis (PsA). A regimen that clears recalcitrant plaque disease may leave inflammatory back pain untouched; an agent that quiets a swollen knee may do little for a patient's dactylitic toe or nail dystrophy. This heterogeneity is precisely why both major guideline bodies now frame therapy around clinical domains rather than a single disease-activity score.1,2
The 2021 GRAPPA recommendations and the 2023 EULAR update both organize treatment by domain while emphasizing that most patients present with several active domains at once, so the goal is to choose an agent that covers as many of them as possible. What follows is a practical walk through the domains and the mechanistic logic that should drive drug selection.1,2
Peripheral arthritis
Peripheral arthritis remains the most thoroughly studied domain and the usual point of entry. EULAR advises rapid initiation of a conventional synthetic DMARD – methotrexate preferred – reserving NSAID monotherapy for mild, short-term disease and explicitly discouraging oral glucocorticoids.2
When csDMARDs fail, or polyarticular disease with poor prognostic features is present, the field opens to TNF inhibitors, IL-17A and IL-17A/F inhibitors, IL-12/23 and IL-23 inhibitors, JAK inhibitors, and PDE4 inhibitors, all of which carry strong recommendations for this domain.1
Because efficacy here is broadly comparable across biologic classes, the differentiating decisions are usually made elsewhere – in the other active domains and in the comorbidity profile.
Axial disease
The axial domain is where mechanism matters most and where the evidence is most contested. In the MAXIMISE trial, secukinumab was superior to placebo for ASAS20 response at 12 weeks in patients with axial manifestations of PsA. IL-17 inhibitors do carry a risk of worsening any underlying inflammatory bowel disease, such as Crohn’s or ulcerative colitis, which have the same genetic risk factors as psoriatic arthritis. On the other hand, IL-23 inhibitors do not seem to carry this same risk.3
TNF inhibitors and JAK inhibitors are likewise reasonable choices for predominant axial disease. IL-23 inhibitors are an open question. Because p19 blockade failed in ankylosing spondylitis, guidelines have been cautious about extrapolating to axial PsA – yet a post-hoc analysis of DISCOVER-1 and DISCOVER-2 showed guselkumab produced greater BASDAI and ASDAS improvement than placebo in patients with imaging-confirmed sacroiliitis.4
The debate over whether axial PsA and axial spondyloarthritis are immunologically distinct enough to justify IL-23 use is now active in the literature. For now, a patient with dominant spinal involvement is more defensibly placed on an IL-17 inhibitor, TNF inhibitor, or JAK inhibitor.5
Enthesitis and dactylitis
These domains track closely with one another and with the IL-23/IL-17 axis. IL-17 inhibitors, IL-23 inhibitors, JAK inhibitors, and TNF inhibitors all show meaningful benefit, and the systematic review informing the 2023 EULAR update confirmed efficacy across these classes.6
Guselkumab, for example, drove higher rates of complete enthesitis and dactylitis resolution than placebo in the DISCOVER program. Practically, the presence of active enthesitis or dactylitis rarely changes the choice on its own but reinforces a move toward an IL-17– or IL-23-based agent.4
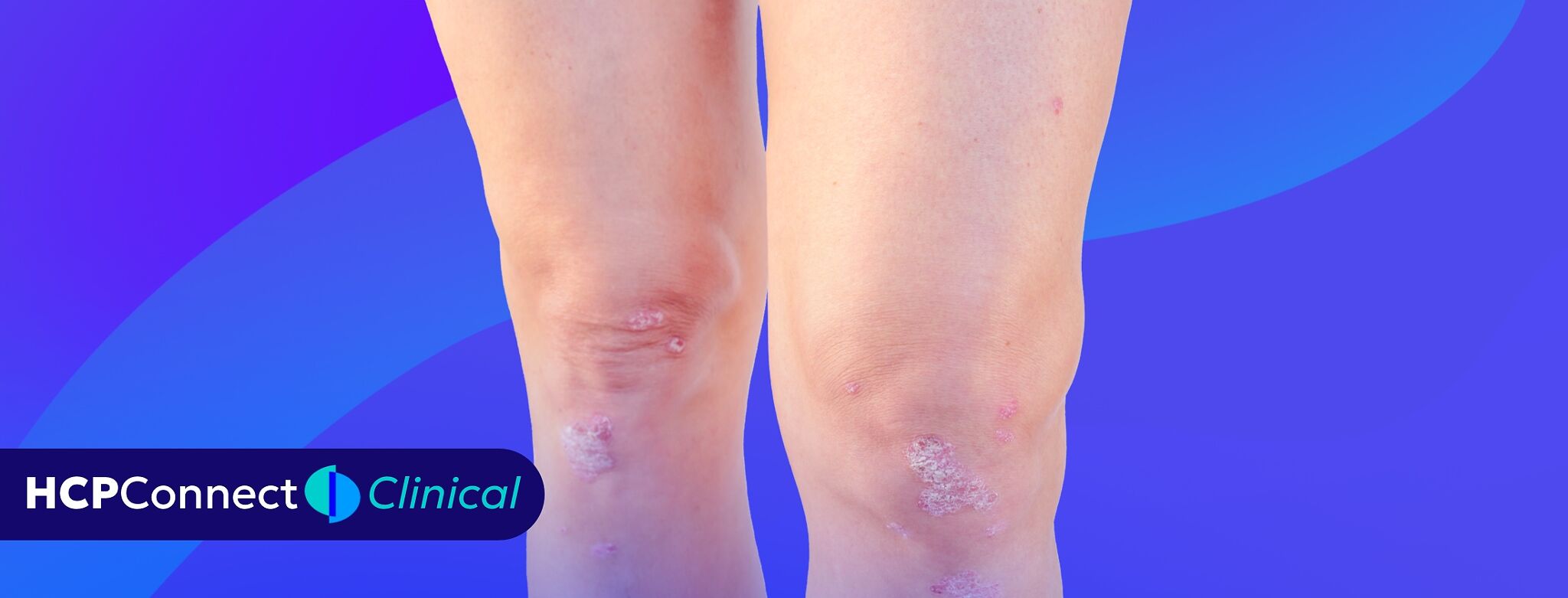
Skin and nail disease
When cutaneous psoriasis is moderate-to-severe, the skin domain often becomes the deciding vote. IL-23 and IL-17 inhibitors carry the highest-quality evidence for skin clearance and generally outperform TNF inhibitors on PASI endpoints, making them the natural pivot for the patient whose joints and skin are both demanding attention.1
Letting comorbidities break the tie
Where domain coverage is otherwise equivalent, safety and comorbidity should decide. TNF monoclonals are favored for concomitant inflammatory bowel disease or recurrent uveitis, whereas IL-17 inhibitors are best avoided in IBD because they can exacerbate it.2
JAK inhibitors warrant caution – and shared decision-making – in older patients or those with cardiovascular or malignancy risk factors, following the safety signals from the tofacitinib ORAL Surveillance trial.7
A comprehensive approach
Domain-based prescribing reframes the central question from "which drug is strongest?" to "which mechanism covers this particular constellation of manifestations most completely and most safely?" Map the active domains, weight axial and skin involvement heavily because they most sharply discriminate between classes, then let comorbidities arbitrate among equivalent options.
Done deliberately, this approach turns PsA's heterogeneity from an obstacle into the very logic that guides rational, individualized therapy.